

This post was originally my comment to a person on Facebook, which somebody then deleted. This person repeatedly throws out the 1.2 M deaths worldwide number and I finally lost it and posted a response to him after he scolded people for “spreading disinformation and not listening to science”. He actually told people disputing the Second Wave Hysteria to “shut up and listen to the government and science”.
As one of my all-time favourite economists, Thomas Sowell, would say…. “Oh dear, where to begin?”
1 million or 1.2 million deaths worldwide sounds like a big number and on its own you can use it to club “Covidiots” into silence, that is, until you actually look at it.
For starters, bandying out a number, any number in isolation is meaningless. For any number to have any relevance, to anything, it has to be part of a data set or otherwise part of some meaningful comparison.
If we take the 1.2 million COVID deaths worldwide, at it’s face (more on that below), the obvious question then becomes “is that good or bad?”
The most useful signal we can get from a global COVID death toll is how it compares to what is called the “Absolute Fatality Rates” globally, which is simply the rate of all fatalities from all causes.
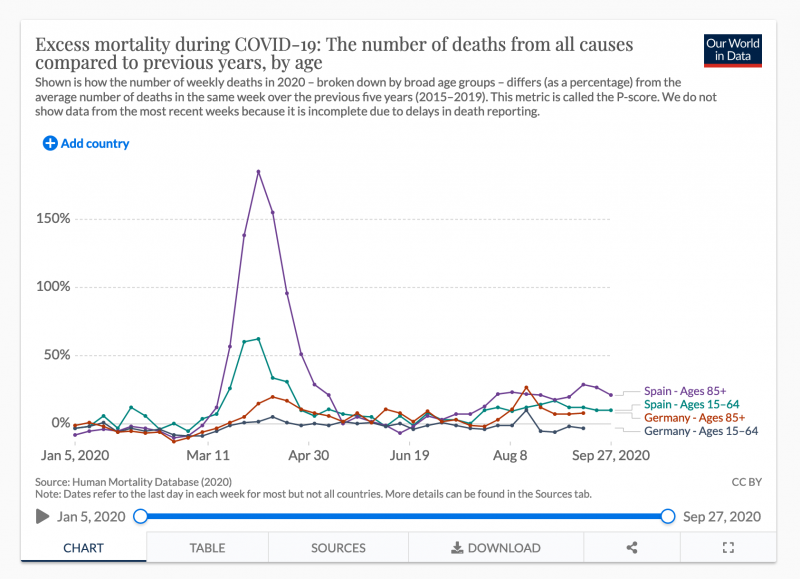
From the charts, we can clearly see, there was a lot of excess mortality in March and April, and then, like every other meaningful metric around Coronavirus, it drops off drastically and starts to level out, with a slight seasonal rise as we head into the winter.
Interestingly, in “no lockdown” Sweden, it turns out their absolute death toll is much lower than one would think:
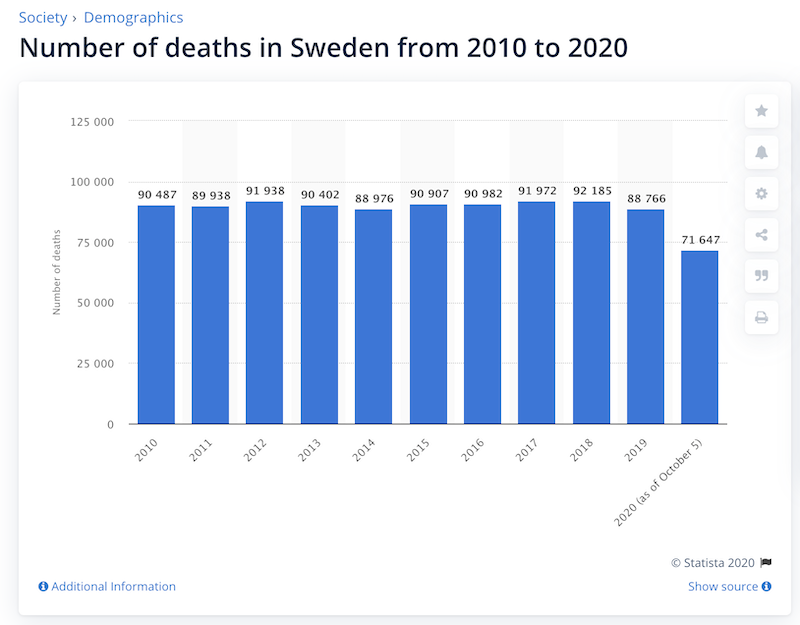
It could possibly come in lower by the end of the year, but if not, will come in not that much higher. Not as high as, say, the US or England.
If reducing fatalities is the goal, there is a much easier way to do that
Sadly, a lot of people die every day, and I’m sure you’ve seen memes on social media on how many more people die from other causes like Tuberculosis (1.4M in 2019) than COVID-19.
In the US, where the COVID death toll currently sits at 225K, it is estimated that medical malpractice kills 250K Americans a year.
But an even bigger number, according to the WHO, is that alcohol abuse kills 3 million people annually, and that number will surely go even higher this year given the massive spike in mental illness, domestic violence, child abuse, depression and suicide caused by the lockdowns.
If this is about saving lives, we could literally bring those alcohol related deaths to zero, turning it off like the flick of a switch by instituting a global ban on alcohol. We could do it tomorrow. Should we? The lives we save may include your own.
In fact if we banned alcohol then we could let Coronavirus run and still be ahead nearly 2M preventable deaths annually, provided COVID-19 kept going with the same intensity it was going in March and April, which it clearly isn’t (see below).
Of course, nobody would seriously entertain that, and they could probably articulate some decent logic around why we shouldn’t.
But they may dismiss it without considering how closely the lockdown approach toward reducing COVID fatalities is analogous to a worldwide ban on alcohol to eliminate alcohol related deaths would be. Especially since we also know that a large portion of coronavirus fatalities die with COVID-19 and numerous other comorbidities* than of it (however, see my footnote on that at the end of this post).
In that sense, alcohol related carnage is very similar. Few alcoholics drink themselves to death outright. Far more kill themselves (and others) in car accidents, commit suicide, or wreck their livers, hearts, kidneys, brains or generally run themselves down so low nearly anything else will finish them off.
Second Wave Hysteria
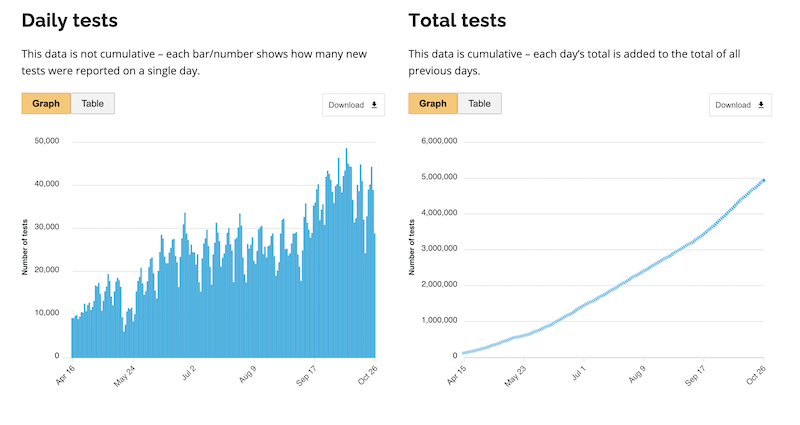
Case counts are clearly rising again globally, that much is true and we have oodles of data to track it. With it, there come fears of the dreaded “Second Wave” of fatalities.
In the often cited Spanish Flu of 1918, the bulk of the fatalities came in the second wave. However, the Spanish Flu was a very different pandemic than the one we have today. That one attacked people right in the early years of the prime-of-life age curve:
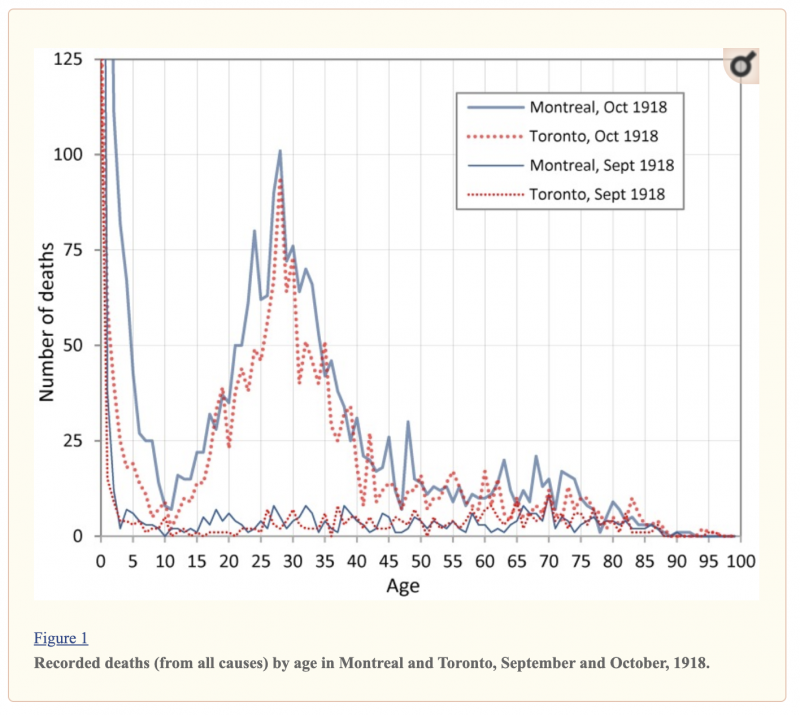
Scientists believe the nature of that strain caused “cytokine storms”, the phenomenon where the immune system overreacts and attacks itself. In a perverse twist of fate, this made the population with the strongest immune systems more vulnerable to the flu.
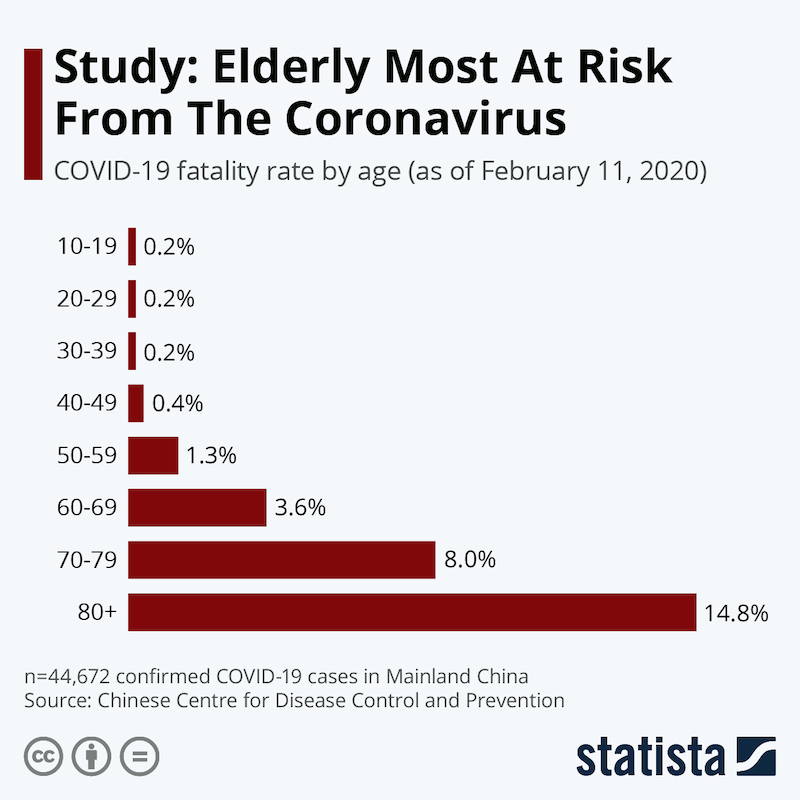
Contrast with COVID-19 where nobody disputes that the most vulnerable members of the population are the elderly and those with underlying medical conditions that render them immuno-compromised. In this sense, comparing 1918 to COVID-19 is not accurate or useful.
So, bear this in mind as I put in the graph below of how the Coronavirus Second Wave is playing out when it comes to case counts vs fatalities:
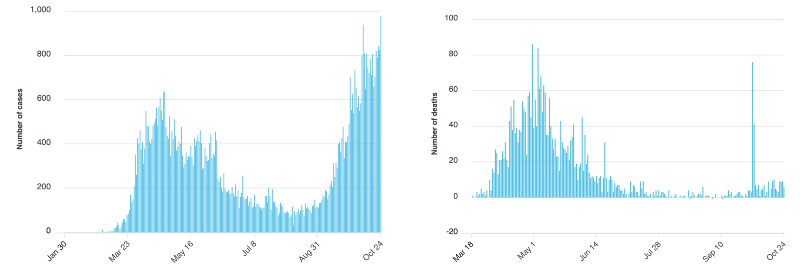
If we were in for a 1918-style Second Wave fatality overrun, we would see it in the data. As I pointed out in my previous post, the above data comes from the Province of Ontario, but pretty well all graphs from locales undergoing second waves in case counts, look the same. The fatalities are riding the floor (that “spike” in the fatality count was a data correction where they took previously missed data from the proceeding 90 days, and added them all to 2 data points), but the case counts are going up, as are the number of tests.
Right now the slope of the case count far exceeds the slope of the fatalities.
For the fatalities to come in anywhere near the Second Wave of 1918 scenario, the slope of the fatality line needs to blast off in a near vertical line right now. In the Ivor Cummins interview he mentioned Dr. Sunetra Gupta’s work indicating that COVID seems to peter out when it hits 20% of the population (but I can’t find the cite). If true, it is hard to envision a scenario where that is mathematically possible.
If not true, and we’re about to experience a Second Wave of fatalities, it would be impossible to occur without seeing it in the data and right now, all of the data, everywhere is showing either a moderate rise with seasonality, or an aggregate, overall decrease in fatalities.
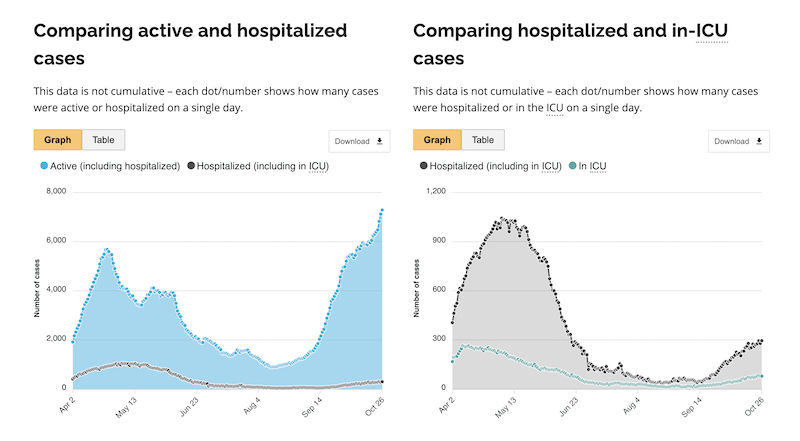
It’s also been pointed out that the rationale behind the lockdowns was to prevent the healthcare system from being overrun. Aside from a few notable exceptions in Phase 1, that didn’t happen. If we look at the data now, it doesn’t look like that’s going to happen now, either. When I first started posting about the second wave numbers, I pointed out that even the ICU cases line was diverging from the hospitalizations line (right side, below). Right now it looks like the total hospitalizations are lower in Wave 2, then they were in Wave 1, even against a case count exceeding previous highs.
All of this should be good news, but for some reason, people become very upset when you try to walk them through this. I’m open to all logic, data and science based objections or counter-points to where I am wrong on this, bearing in mind that “SHUT UP AND LISTEN TO THE GOVERNMENT AND SCIENCE” isn’t a logical, scientific or data driven counter-argument.
What to do next.
I would close out with two additional reading exercises, one, I would go look at The Great Barrington Declaration and if you think they’re approach of focused protection makes sense, sign it. Number two: have a look at the comparison of The Great Barrington Declaration with what’s called “The John Snow Memorandum“.
If you want to follow my work, and I seem to be covering more about the lockdowns lately, then sign up for the mailing list here, or follow me on Twitter here.
Footnote on Comorbidities
(*The number you see bandied around a lot is 94% of all COVID-19 fatalities had comorbidities. This number largely keys off CDC data that only 6% of fatalities list only COVID-19 as a c.o.d. If you look at the CDC data on what the comorbidities are, the biggest one accounting for close to half of all fatalities, especially in the elderly, is pneumonia and influenza. I think it’s inaccurate to just net-out all of those cases and dismiss them as comorbidities because that is one of the most common ways respiratory viruses manifest. But that said, the data, when you consider comorbidities and the looseness with which COVID gets added to c.o.d’s, what all this means is that the headline number for fatalities is the top boundary. They aren’t higher, and they are probably for all practical purposes, lower).
While comparing the number of C19 deaths to other types of deaths makes it look lie everything else, but what is missed is that the spikes like we are experiencing now overwhelms our health care systems. This overwhelm makes it difficult to treat the other medical needs of the population. Wearing masks and practicing social distancing can keep the spikes from occurring, or at least levels them out enough to not overwhelm those systems.
I’ve been following the ICU stats for Ontario and talking to people I know in the healthcare space – while metro Toronto has gotten a little loaded at times, for the most part ICUs are empty. There is plenty of capacity.
There were a few notable areas worldwide where ICUs were overrun in Wave 1 but for the most part, health systems held up just fine.
We could easily end the pandemic by using the known safe & effective treatments: Vitamin D, ivermectin, HCQ+zinc, chlorine dioxide, niacin… But no, let’s mask up, lock down, destroy economies, wait for liability-free experimental vaccines because “hospital capacity might get overwhelmed”… makes sense.
There is no evidence that the health service was overwhelmed in the majority of western countries, so social lockdown policies was totally ineffective in retaining access to medical care. In the UK, and many other countries access to non Covid 19 issues was reduced when the hospitals were cleared to make room for the non existent rush of Covid 19 patients, while bed occupancy was at historic lows in the UK, and nightingale hospitals were mostly unused, while attendance at A&E for heart attacks was down by half with significant reduction in cancer screening and treatment, and a number of conditions far more serious than Covid 19.
It was the lockdown, not Covid 19 that reduced access to medical care. In reality the lockdowns have killed far more than Covid 19 and will kill people for decades to come from withdrawal of medical treatment to increasing poverty. There is also no reliable evidence that masks are effective in treating airborne respiratory viruses infections, and a considerable body of academic literature suggesting little if any effect. Sweden that didn’t practice significant social distancing did not experience a more significant spike in deaths in comparison to lockdown countries (see our world in data and FT data below), and has the 15th highest per capital Covid 19 deaths in the world, and does not have particularly high overall excess deaths over this period (FT again).
I am sorry about the UK centred nature of this data, but I am more familiar with it, but similar things happened as the UK in many countries, such as New York, Italy and Spain, where hospitals emptied old vulnerable unscreened people into care homes where Covid 19 was hot housed and medical treatment was denied as part of the lockdown strategies.
https://www.hsj.co.uk/acute-care/nhs-hospitals-have-four-times-more-empty-beds-than-normal/7027392.article
https://www.bhf.org.uk/what-we-do/news-from-the-bhf/news-archive/2020/april/drop-in-heart-attack-patients-amidst-coronavirus-outbreak
https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938
https://ig.ft.com/coronavirus-chart/?areas=usa&areas=gbr&areas=swe&areas=bel&areas=esp&areas=ita&areasRegional=usny&areasRegional=usca&areasRegional=usfl&areasRegional=ustx&byDate=0&cumulative=0&logScale=0&perMillion=1&values=deaths
https://ourworldindata.org/grapher/excess-mortality-p-scores?tab=chart&stackMode=absolute&country=ESP~DEU~NOR~FRA~ITA~NLD~BEL~CHL~SWE~GBR~USA®ion=World
https://www.statista.com/statistics/1104709/coronavirus-deaths-worldwide-per-million-inhabitants/
https://www.telegraph.co.uk/news/2020/07/19/lockdown-may-cost-200k-lives-government-report-shows/
RR619 Evaluating the protection afforded by surgical masks against influenza bioaerosols
https://www.hse.gov.uk/research/rrhtm/rr619.htm
Looking at the numbers you publish, may I ask, “Is the Pandemic the first salvo of the coming collectivist’s revolution to lynch the last of the individuals?” The collectivists will win in time (because all the influential philosophers pray for it and extoll its mythical features), but not yet.
My first clue that someone was lying last March was when the media failed to differentiate between the victims as DYING OF and DYING WITH the pandemic. The devil is always in the details which the irrational always obfuscate.
All those Covid-19 positive tests don’t mean what most people suppose. The test looks for a target viral RNA fragment. What is more, to get something testable from a sample, typically many cycles of PCR are undergone to multiply the number of copies of RNA fragments. There is a lot to go wrong if it is not done carefully, but leaving that aside, let us assume that the target fragment matching is 100% accurate. Does that mean that all those positive tests indicate infectious people with active virus?
1. Active virus? no way to distinguish between a fragment derived from currently active virus and a left over fragment from dead virus.
2. If active virus present at time of sampling, is the person infectious? Not enough data to know the degree to which a symptom free person, who never develops noticeable symptoms is infectious. The data from young children indicates very little transmission of infection from them to adults such as their teachers or family members.
Bottom line: It is completely dishonest to call those positive-for-fragment tests “cases”. If you were to use the case criteria we use for every other illness, the case incidence in the community in this “second wave” would be negligible.
Yep, and you can find these fragments in pretty much everybody by merely doing enough cycles. A cycle threshold (Ct) above 33 cycles is already problematic as admitted by the NYT and even the GoF-man pHarma chief himself, Fauci (see for yourself at watch?v=a_Vy6fgaBPE&t=260). Yet, FDA still has it at Ct=40. In fact, it can be easily seen that the Ct value is DIRECTLY PROPORTIONAL to the level of criminality displayed by each government. Most seem to use 40 at most because above that you just start getting absurd amounts of “positives” (which only a dangerous criminal would call “cases”). I hear the UK is using 45 cycles and only because the enzyme (DNA polymerase) breaks, imagine that…
The problem with the idea of “herd immunity” is that there is no evidence at all that it is possible. We have evidence of people being infected twice within a few months. And if you look at the numbers in Spain, you’d expect them to have developed herd immunity in Madrid, looking at the numbers of infections in the first wave. But they’re getting a second wave that is pretty high, so no evidence of herd immunity there.
So, if herd immunity may not even be possible, it makes sense to keep some level of restrictions till there is a vaccine. After all, why take any risk of overwhelming hospitals? Now, different reasonable people may have different opinions on what level of restrictions is best. But saying that the best is no restrictions at all seems to me pretty reckless.
I think you need to revisit the concept of herd immunity – it of course does occur and there is strong evidence in places like NYC – very few actually get reinfected – like a rare rare event that could also be tied to issues related to testing procedure errors- the second wave is a known fact of seasonal flu viruses and efforts to suppress the first wave gave rise the the nature of the second and likely much lower 3rd wave of this flu – if anything, our efforts to reduce the 1st wave only made the second one stronger. The whole ide of the health program was to reduce the 1st wave to take pressure off hospitals – a complete error.
If you have a problem with the idea of “herd immunity” based on the reasons you stated, how can you look towards a vaccine as a solution? It would seem that what you are saying is the body is not capable of building it’s own defense and must therefore rely on a synthetic approach. Suffice to say, I am extremely skeptical of that line of reasoning.
That makes absolutely no sense as a vaccine works by using a live or denatured-virus to trigger ones immune response. If it is impossible to develop any long term immunity from natural exposure, then any vaccine will not give any kind of long standing immunity so would also be ineffective.
A good example of this is the flu vaccine, that has to be changed each and every season and is fairly ineffective as flu mutates even more than Covid 19, that is a variant of the common cold virus that too date no one has successfully developed a vaccine for. A vaccine is only useful where exposure to the virus to develop immunity is unsafe, this is not the case with most people with Covid 19, so would be useful only if properly tested for efficacy and safety over a similar long time period as other vaccines in common usage, as such if one existed that was safe it would only be useful for those who cannot be safely exposed such as the old and with pore existing conditions.as an adjunct to naturally acquired immunity to reach herd immunity. A vaccine works only by reaching heard immunity more safely where exposure to the live virus is not safe, such as polio or smallpox, Spanish flu would also be a candidate if it still existed, as it attacks the young and healthy, unlike Covid 19.
I have seen no good evidence for widespread secondary infection, given the poor reliability and unsuitability of PCR testing, that was never designed for diagnostic testing as the number of replication cycles will determine whether you get a positive result, where dead remnants of a Covid 19, long after recovery or similar will test positive.If you have any good reliable information about re infection could you link to it?
Re-positive coronavirus disease 2019 PCR test: could it be a reinfection?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7439804/
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600%2820%2930453-7/fulltext
Testing faults blamed for South Korea coronavirus reinfection results
https://www.sciencefocus.com/news/testing-faults-blamed-for-south-korea-coronavirus-reinfection-results/
No, it makes absolutely no sense “to keep some level of restrictions till there is a vaccine”. I guess you haven’t noticed that they’re suppressing all effective treatments (vitamin D, ivermectin, HCQ+zinc, niacin, CDS, NAC…). While pushing useless remdesivir to make it look like we have no effective treatments hence only a vaccine can “save” us.
Indeed, according to Stats Canada, 283,706 people died in 2018, from all causes. This would average to about 23,642 per month. At its worst in April 2020, how many died (apparently) from Covid, about 5,000 or 6,000?. Total is now just under 10,000? Doesn’t a bad influenza season usually kill about 8000? So, if we remove the 75 per cent dead in long care and elderly facilities, where it seems most died not directly from Covid, but likely from dehydration, starvation, and deadly sores caused by not having diapers changed for 2 or 3 weeks (PSW’s apparently were so terrified of Covid that they refused to help these poor tragic people), then about 2,500 have died from Covid. This is much lower than a bad influenza season!
Is this really just that infectious disease experts around the world are finally having their day in the sun, so to speak, and now they and these duped politicians (I’m looking at you Dr. Tam, Dr. Williams, Mr. Trudeau and Mr. Ford)can’t admit they were wrong and so are perpetuating this crisis?
I have, like you taken a look at the data for a long time with an objective to open a couple of eyes along the path. Human population adds more than 60 million net every year and given the natural mortality curves we also have to have >1% of total population of 7.8 billion of us die every year. All about as straight forward as we can be without even understanding simple math. Your article recaptured this reality in a good way and serves as another reminder to people.
You will find a 2008 article by Fauci interesting because he and a colleague looked at the Spanish Flu and came to the conclusion that most deaths were caused by pneumonia bacteria, that can be the secondary effect of the cytokines storm you referred to, but that they also believed that masks contributed substantially to the rapid outbreak of pneumonia.
I also have produced the statistics from events we knew last March and April that showed us the true expected death profile of the corona virus basically from the Diamond Princess, Charles de Gaulle and Teddy Roosevelt aircraft carriers plus the front line workers in NYC (another most interesting case).
All this aside, for me the real area of interest is human behaviour and decision-making processes that have led to the management routes taken to date and those continually being proposed going forward that are driven down our throats despite the science that says we will be just fine. All of human history is about mass hysteria of one sort or another – it is what we are and hoping for change in human behaviour at large community scales is a pipe dream in the absence of a check and balance decision-making system – your reference to sweden is excellent and there are several other political jurisdictions around the world that serve as further supportive evidence that most of the world took exactly the wrong path.
I will not sign the Great Barrington Declaration until they remove the obvious POISON PILL that continues to recommend the use of the fake PCR test.
The PCR “method” has been exposed by many, including inventor, Kary Mullis himself, as a method that has no ability to detect an infectious coronavirus.
COVID-19 is a PCR test Pandemic having nothing to do with a lethal coronavirus. Video from Reiner Fuellmich, Kary Mullis and series of articles by Jon Rappaport https://bit.ly/36L8ntq
I thought this was a very good article. But the following made me laugh. “If this is about saving lives, we could literally bring those alcohol related deaths to zero, turning it off like the flick of a switch by instituting a global ban on alcohol. We could do it tomorrow. Should we? The lives we save may include your own.” As if governments banning something makes it go away! What is that old saying about the only thing we learn from history is that we learn nothing from history? If the 1920’s prohibition of alcohol taught us anything it’s that Governments banning something doesn’t make it go away.
I meant to put a “presumably” in there.
That would have helped. But there are plenty of people out there that believe that Gov banning something is a solution. As we should learn from the Prohibition of Alcohol in the US, people will find a way to get what they want regardless of laws. It’s true of any prohibited substance like cocaine, marijuana or heroin. In many places they are out right banned yet available on the black market. Unfortunately the black markets come with high crime. It’s the unintended consequence of Gov’s banning something people want.
That whole example was supposed to be reductio ad absurdum.
Today, it seems that the absurd is in vogue. It’s often hard convey the reductio ad absurdum accross via the written word. I have seen many people seriously submit Gov banning of something as a solution. A current example would gun bans. I have tendency to take things a face value.
I found this reference to the estimate of herd immunity of 10-20%, (that refereed to Sunetra Gupta’s estimation in the article;le above. stating that it missed a reference) not peer reviewed, but then again neither was the Neil Fergusson paper providing justification for lockdowns.
Aguas, R., Corder, R.M., King, J.G., Goncalves, G., Ferreira, M.U. and Gomes, M.G.M., 2020. Herd immunity thresholds for SARS-CoV-2 estimated from unfolding epidemics. medRxiv.
https://www.medrxiv.org/content/10.1101/2020.07.23.20160762v2
States “Our inferences result in herd immunity thresholds around 10-20%, considerably lower than the minimum coverage needed to interrupt transmission by random vaccination, which for R0 higher than 2.5 is estimated above 60%.”
Also a article in the BMJ, refers to the study above
“Covid-19: Do many people have pre-existing immunity?”
https://www.bmj.com/content/370/bmj.m3563
“while most experts have taken the R0 for SARS-CoV-2 (generally estimated to be between 2 and 3) and concluded that at least 50% of people need to be immune before herd immunity is reached, Gomes and colleagues calculate the threshold at 10% to 20%.2223”
1918 Spanish Flu mortality chart for Toronto-Montreal.
The absolute mortality numbers for the 90+ age group was very low, but how many people were there over 90 years old in 1918 in these cities ? This chart is not very meaningful in absolute numbers, more meaningful would be mortality as a percentage of the total population of each age group.
In a press conference a couple of weeks ago the WHO said, that 10% of the current world population, i.e. 780 mio are infected. At the same time the WHO death count as of today is 1,155,553. So, anybody could do the simple math and divide the latter number by the first: 0.148 percent! No conspiracy theory required.
In Kansas, USA, they’ve been caught juicing the stats – “The New York Times reported in August that some of the nation’s leading public health officials say the standard COVID tests with cycle thresholds at 40 or higher are “diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus.” Virologists and most researchers, including the Centers for Disease Control, agree that it is difficult to find live virus capable of transmission beyond 34 cycles. But the Kansas state lab, which conducts about 24% of all tests in the state, is using a cycle threshold of 42 cycles and likely finding dead virus particles that can’t be transmitted to others.
The Sentinel found private labs are also using cycle thresholds above virus viability. Quest Diagnostics, in Lenexa and Salina, sets their cycle threshold at 40. LabCorp, in Kansas City, KS, Kansas City, MO, Lawrence, Overland Park, Salina, and Wichita, sets their PCR test to a cycle threshold of 38.
Michael Mina, an assistant professor of epidemiology at both Harvard Medical School and the Harvard T.H. Chan School of Public Health told Harvard Magazine that reporting someone positive on a test with a high cycle threshold is like finding a hair in a room, testing it for DNA, and then saying the person who shed that hair is currently in the room.
“That’s a false positive, but that’s what we’re doing,” he said.” https://sentinelksmo.org/kansas-labs-set-cycle-thresholds-too-high-detect-non-contagious-virus/
and stonewalling about it – “As reported last week by the Sentinel, many labs are setting the cycle threshold on COVID tests above the recommended level, which, according to CDC calculations and many virologists, will produce false positives by detecting non-contagious particles. The Sentinel sent an Open Records request to Johnson County seeking the cycle threshold for every positive result in the county but officials said “the disease reporting system maintained by the Kansas Department of Health and Environment, does not contain cycle threshold data.”
In a series of follow-up questions, we asked if health officials, County Manager Penny Postoak-Ferguson, or county commissioners would like to have KDHE provide the cycle threshold information for past and future tests and if such a request will be made. We also asked if they believe the cycle threshold should be set no higher than 34 as suggested by the CDC and many virologists.The emailed response on behalf of the county from Deputy Legal Director Cynthia Dunham said, “We have nothing further to add to our prior response to your KORA request.”
County Commissioner Mike Brown, however, sent his own reply.
“If the testing cycle threshold of Johnson County does not align with CDC guidance, that is wholly unacceptable and must be rectified immediately by Johnson County.”
Each COVID test manufacturer makes its own cycle threshold recommendation, but reporting by the New York Times says setting thresholds too high will detect genetic fragments that are not contagious.
“Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said.
“Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think that 40 could represent a positive,” she said.
“A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on.”
Dr. Michael Mina, quoted above, is an assistant professor of epidemiology at both Harvard Medical School and the Harvard T.H. Chan School of Public Health. He told Harvard Magazine that reporting people positive on tests with a high cycle threshold are “false positives.” https://sentinelksmo.org/joco-officials-dont-know-how-many-covid-tests-may-be-false-positives/
In other words, they’re manufacturing fake statistics to support a political agenda… so if you want to get rid of the “pandemic” get rid of these people, kick them out of office, and don’t put your trust in their lies. So far as credibility goes, they’re finished and they shouldn’t be in positions of power.
And here’s a real solution that requires neither lockdowns, vaccines, immunity passports, or potentially masking – “FOR PUBLIC-HEALTH PURPOSES, speed and frequency of testing are vastly more important than sensitivity: the best test would actually be less sensitive than a PCR test. As Mina explains, when a person first becomes infected, there will be an incubation period when no test will reveal the infection, because the viral loads are so low. About “three to five days later, the PCR test will turn positive, and once that happens the virus is reproducing exponentially in a very predictable fashion.” At that point, critically, “even if a rapid test is 1,000 times less sensitive than a PCR test,” Mina says, the virus is increasing so rapidly that the test “will probably turn positive within eight to 15 or 24 hours. So the real window of time that we’re discussing here—the difference in sensitivity that makes people uncomfortable”—is so small that public-health officers would be missing very few asymptomatic people taking the test in that narrow window of time. Given that the current testing frequency in most states, using highly sensitive but expensive and delayed PCR tests, is not even once a month, he points out—“Really, it’s never.”
So even though a saliva-based paper test wouldn’t register a positive result for as long as a half or even a full day after the PCR test, it would have great value in identifying pockets of infection that might otherwise be undetected altogether.
The strength of this system is that it would actually abrogate the need for contact tracing, says Mina. “If your goal is not to have a heavy hand over the population” (implementing onerous public-health restrictions on businesses and recreational activity), this is the way to do it, he explains, because it strips away “all of that complexity.” Most people who test positive will have done so before they become infectious, and can easily self-quarantine for the six days or so until they cease being infectious. Even if some people don’t quarantine, and the test cuts off just 90 percent of all the infections that might spread, “you’d immediately bring the population prevalence of the disease to very low numbers, to the point where all of a sudden society would start to look safe again.”
MINA HAS BEEN PREDICTING the advent of more widely available, cheaper tests for months. But those tests have not materialized, largely because of regulatory risk, he says: manufacturers cannot meet Food and Drug Administration (FDA) templates for test sensitivity that use PCR as the standard. The FDA—whose approval process is stringent because it is designed to test the efficacy of clinical diagnostics—has no jurisdiction over public-health testing. But at the moment, there is no alternative regulatory process for tests designed to ensure population-level wellness—such as a certification program that might be run through the Centers for Disease Control (CDC), the agency charged with safeguarding the public health.
“It is time to stop allowing diagnostic definitions to get in the way of absolutely essential public-health interventions,” says Mina, for whom explaining the distinction between the two types of test, and the different ways they can be used, has been an uphill battle. But it is one that he desperately hopes to win—and that the country needs him to win—for public-health measures to stand a chance of reining in the outbreak as schools and other institutions move toward reopening this fall.
The U.S. government has spent billions of dollars supporting attempts to develop vaccines and therapeutics. “Developing a good vaccine is very difficult to do,” he points out. “It’s a crapshoot that may or may not work. We’re putting billions more into developing therapeutics [treatments for COVID-19] which is really, really difficult.” With rapid testing, by contrast, “We have solutions, sitting in front of us right now, that are cheaper, would be much quicker to build, and much less risky to actually introduce and roll out. And the only thing standing in the way is that there just doesn’t seem to be the will to bring a public-health tool to market.” https://harvardmagazine.com/2020/08/covid-19-test-for-public-health
I would be interested in seeing total deaths from ALL causes (in numbers; not percentages) year over year to see the true spike in total deaths year over year specifically from Covid. Did you happen to run across that data? Thx!