

In part 1 I talked about two COVID-19 / Great Reset themed conspiracy theories that were spreading in Canada and why embracing or amplifying them made lockdown skeptics look like lunatics who could more easily be dismissed.
There is no shortage of science and data to challenge the flawed policies of the governments whose basic playbook has been: lockdown, close economy, print money, ignore data, and double down.
This may be a good time to quickly outline my arc of how my views on the pandemic shifted over time.
My journey from Zombie Apocalypse to lockdown skeptic
I began monitoring the reports of a new virus emerging out of China in January. On January 23rd I emailed a friend advising him to go out the next day and pick up some N95 masks. By the first week of February I was stocking up on food, medical supplies, cash, and weapons while advising friends and family to do the same. I was bracing for a full breakdown of the global supply chain and a collapse of the global economy.
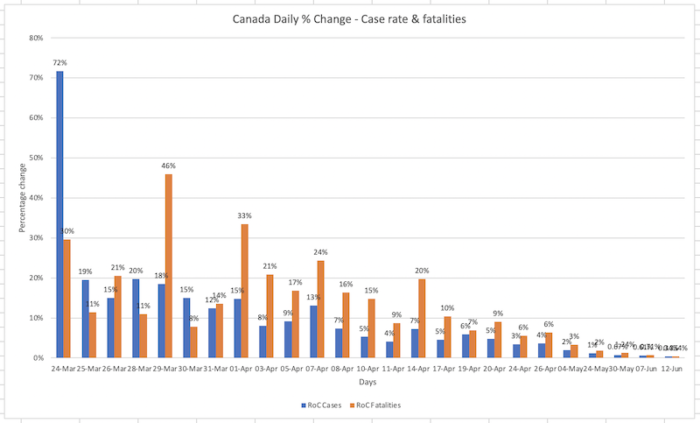
Based on early reported numbers of an R0 around 3.1 with an IFR of 5%, it looked like we’d see doubling times of 15 days. By March all three levels of government, city, province and national were reporting case rates and fatalities daily. I put together a spreadsheet and using those numbers as a model I forecasted Toronto to have 1.7M cases by the end of June. If the IFR really was 5%, or even 3%, it would mean between 51,000 and 136,000 fatalities.
This was terrifying, so as the world started locking down, it seemed to make sense. In fact I was wondering why we were still allowing inbound flights from hotspots like China? There were rumblings from The Clerisy like the New York Times that blocking flights from China would be racist. This was the early innings of the politicization that was to follow.
But then, a curious thing happened. The rate of change in infections and fatalities started coming down, drastically.
By June it was clear to anybody following the data that this was, at least for now, largely in the rearview mirror. I had been in touch with an old friend who now ran IT for several hospitals. In January he was trying to get administrators to take COVID seriously. By May, they had built 4 additional ICU wards across their hospitals and they were sitting empty. Worse, resources were being denied to other medical uses. He was beginning to wonder if maybe this wasn’t going to be as bad as we both originally thought.
Then, over the summer despite the clear slowdown in the severity of the pandemic, the policy response to it intensified. And then it all became political. Questioning the efficacy of continuing the lockdowns became associated with being alt-right. Pro-Trump. Or worse. A Narrative War ensued. If you questioned official policy, you got deplatformed. I documented numerous instances of this over on AxisOfEasy.
Now we’re in the fall and the case counts are back up and Second Wave Hysteria is in full effect. The only problem is, the fatality rate is on the floor. Another problem is this shouldn’t be a problem. It should be good news!
The fatalities are up slightly with the season, but nowhere close to tracking the case counts as they did in wave 1. This could be for a number of reasons (more testing, the most vulnerable were hit in wave 1, etc) but no matter how you slice it, the graphs pretty well everywhere look like this:
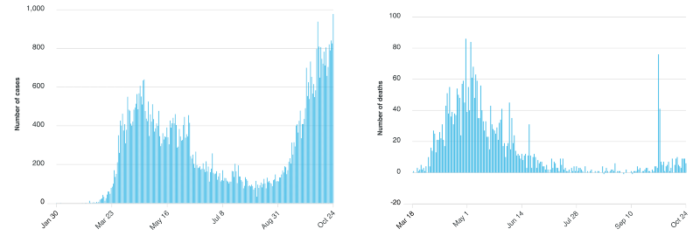
In this case, we’re talking about the Province of Ontario, which has to date nearly 70,000 cases total and slightly over 3,000 deaths. Nothing like the 1.7M cases and 50K to 136K fatalities my original model predicted for Toronto alone.
What does that mean?
It means my model was wrong!
Which is ok, and fortunate, in fact. Now I’m not an epidemiologist, so I’m allowed to get my models wrong. But what I did do, that policy makers and experts are not doing, is re-examining the premises in the face of new data.
The Imperial College / Neal Ferguson model that inspired much of the global lockdowns is an extreme example of this. It turned out to be total shitcode, but it hasn’t impacted the policy response. Not one bit.
There is no justification for more lockdowns
Which brings us to the Triggernometry podcast I mentioned in Part 1, which I never did get around to adequately summarizing. It’s a great conversation with those merry comics Konstantin Kisin and Francis Foster and their guest this episode: biological engineer Ivor Cummins.
When you challenge the prevailing orthodoxy around anything COVID, it’s not uncommon for people to hysterically shriek at you that have to follow science and look at the data! Well, that’s what Cumins has done and here’s the upshot of what he (and many others) have found:
- We should not have locked down over the summer. With cases and fatalities down it was the ideal time to let the virus spread amongst the low risk population to get further toward herd immunity.
- Forcing mask wearing at the nadir of the pandemic (the summer) was a flawed policy that leaves no exit strategy. We’re basically in masks forever now.
- 40 years of published science indicates that masks (especially surgical and cloth masks, as opposed to N95) don’t make much of a difference when it comes to these types of pathogens, but four or five hastily rushed papers from over the summer of this year say otherwise.
- The argument against pursuing a herd immunity strategy because of the so-called “long timers”, people who get COVID, and experience ongoing, long term and possibly life long effects is not a compelling argument. Statistically these cases are low, but more importantly they are not unique to COVID-19. We always have these edge cases with long term effects in seasonal flus and other diseases.
- The fatality curve is playing out along established patterns regardless of whether their were lockdowns or not.
- The first lockdown was understandable. A second one is completely unjustified.
Unfortunately what has happened is this has become about politics and ideology instead of public health. The real world, long term health effects of lockdowns and a crashed economy, the mental health issues, suicide, domestic violence and substance abuse are very real, and have now surpassed the damage being caused by the virus itself. I seem to remember two doctors in California who warned this would happen who were deplatformed and vilified for saying it.
The science and the data are out there, but those who push it forward are frequently accused of “reading what they want to see in the data”. If you revisit the two charts I posted above, that clearly show how case counts have diverged from fatalities, which are flat, I was told exactly that by people when I posted those charts a month ago.
Them: You’re just seeing what you want in that data.
Me: Aren’t these two curves clearly diverging, and one is flat?
Them: Just wait two weeks.
Me: Aren’t you literally extrapolating what you want to see in the data by saying that?
Them: These alt-right denialists are too much.
Well the two weeks, four weeks, six weeks everybody keeps telling me to wait for their extrapolation to kick in have come and gone and we can clearly see that the worst of the COVID-19 induced destruction is in the rear-view mirror. If the numbers change and new data emerges that changes things, I will modify my opinion accordingly. That’s the way it’s supposed work.
But we live in an age where policy makers working off of hypothetical models and career politicians with zero real world experience and no economic skin in the game are egged on by billionaire monopolists philanthropists and their pet projects in narcissism “re-imagining society”. They don’t know how to do anything other than double-down on failure while everybody else bears the consequences.
We need to reopen the economy and start picking up the pieces from all the other collateral damage we’ve caused.
Here is the entire Triggernometry video, I highly recommend watching it and circulating it among your colleagues.
Herd immunity is only possible with duration of immunity. Unless there is new data I’ve not seen yet, they aren’t able to show duration of immunity past 60 days. Pandemics will sweep through the globe, and because these viruses are actually not that strong when it comes to mutation and lasting a long time, it will slowly dwindle away by next summer. History repeating itself again.
There are a lot of misconceptions about coronavirus herd immunity. It is worth listening to Dr. Sunetra Gupta on the subject. There are 4 other coronaviruses that are endemic amongst humans. Covid-19 seems to follow a similar pattern. Antibodies fade fairly quickly (n the scale of weeks) and in many cases are not produced at all. Immune memory seems to be mostly via the T-cell system. That memory seems to last for a year or two with the other viruses. There also seems to be a fair bit of cross-strain resistance. That is: if one coronavirus gives you a cold, say, the primed T-cells, confer resistance against other strains of coronavirus.
The above means that antibodies are not very important to defence against coronavirus. It also means that antibody counts are very misleading in judging the prevalence of Covid-19 encounters in the community. That may explain the more-or-less universal experience that the epidemic fizzles once the proportion of the population with Covid-19 antibodies reaches around 20%. This was the case in London, England, and New York City. That fizzling suggests that herd immunity was achieved.
Dr. Gupta talks about achieving endemic equilibrium with Covid-19 (like the other 4 coronaviruses). At that stage, one expects eruptions every few years, but they would be manageable.
Natural immunity, even if temporary, gets a boost from re-exposure to the pathogen. It’s conceivable that social distancing and masking may prevent such a boost, and actually diminishes herd immunity. Public health mandates may actually cause more harm than good in the long run.
Like you, Mark, I have followed the data and science from the beginning, watching every one of Chris Martensen’s updates as soon as it came out. The trajectory of my thinking has closely tracked yours. I locked down my household a full week before it was mandatory. I only got 3 N95s before they became unavailable.
Right after I tweeted this article a blue-check came across my timeline breathlessly misquoting a press release from a San Antonio hospital. The PR described a contingency plan. The plan’s title suggested, and the blue-check stated as fact, that the plan was already being implemented. I get a little nervous about tweeting covid information (and I strive to keep these tweets factual and linked to actual data and science) because I am on Twitter for professional networking purposes. I’ve been called out a couple times for being “insensitive”. Responding with facts results in crickets. At least that is better than an ad hominem pissing match. You would think people in my field, software engineering, would be more data and science oriented and less emotional. Maybe this goes a long way in explaining the quality of most software.
I know first hand of a half dozen individuals and families affected. No one was hospitalized, including elderly (80+) relatives. We fortunately rescued my mother from a convalescence facility shortly before 12 people died of the virus there. So yeah, vulnerable people need protection.
Where we may disagree is on indoor and crowded outdoor mask wearing. I’m more in the something is better than nothing camp. And maybe wait staff at bars and restaurants should be outfitted with N95s for their indoor and full-capacity-allowed protection.
I haven’t seen anyone suggesting distributing portable HEPA air filters in public indoor spaces, and/or UV lights (not directed at people) at ventilation outlets. Seems like that could reduce virus saturation indoors.
To your point on masks, I just mask up in public because if they actually do something, great, if they don’t, who cares. It’s a low cost way to get some optionality. Ideologically I think it’s a dumb hill to die on.
But that said I do worry that it’ll be “masks forever” even after the crisis has undisputedly passed. I have mild asthma and I don’t like wearing them for long stretches. Flights, when they are a thing again, will be a real drag with masks.
Agree that indoor air quality is the one thing that would seem to be a legitimate mitigation strategy that has been totally ignored – have a friend who is in commercial HVAC who has been posting study after study about this, including lessons learned during the SARS outbreak. Yet local health dept has said NOTHING about indoor AQ. Agree we should be focusing on mitigation that would also benefit during flu, etc. But spreading fear = more clicks = more revenue. As for the masks, yeah, something better than nothing, but also can’t help but feeling like wearing a mask communicates, yes I am compliant with the dictates of a health department who said nothing about mass protests, keeping the big box stores open but banning outdoor gatherings that were not protests and allowing small businesses to open.
You make a good point about “masks forever”, as did Ivor Cummins. I hadn’t thought about that angle.
I don’t have much to argue with other than the stance on masks. My experience with efficacy research does not square with yours. Decent overview article in Nature recently indicating that evidence appears to be trending in favour.
https://www.nature.com/articles/d41586-020-02801-8